|
Rationale for Endoscopic
Ear Surgery
Cholesteatoma is usually a manifestation of advanced
retraction of the tympanic membrane that occurs when the sac
advances into the tympanic cavity proper and then into its
extensions such as the sinus tympani, the facial recess, the
hypotympanum, and the attic. Only in advanced cases, which
now occur rarely, does a cholesteatoma progress further to
reach the mastoid cavity proper. Most surgical failures
associated with a postauricular approach seem to occur
within the tympanic cavity and its hard-to-reach extensions
rather than in the mastoid. Therefore, the most logical
approach to the excision of a cholesteatoma involves
transcanal access to the tympanic membrane and tympanic
cavity and the subsequent step-by-step pursuit of the sac as
it passes through the middle ear. In the past, mainstream
ear surgery has usually involved the mastoid and the
postauricular approaches because operating with the
microscope through the auditory canal is a very frustrating
and almost impossible process, especially when the sac is
excised from the mesotympanum. The view during microscopic
surgery is defined and limited by the narrowest segment of
the ear canal.
 This
basic limitation has forced surgeons to create a parallel
port through the mastoid to gain keyhole access to the
attic, the facial recess, and the hypotympanum. This
basic limitation has forced surgeons to create a parallel
port through the mastoid to gain keyhole access to the
attic, the facial recess, and the hypotympanum.
In
contrast, transcanal operative endoscopy bypasses the narrow
segment of the ear canal and provides a wide view that
enables surgeons to look “around the corner,” even when a
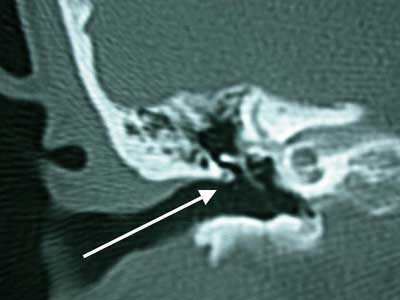
zero-degree endoscope is used (Figure 2). Another anatomic
observation that supports transcanal access to the attic,
which is the most frequent auricular site of cholesteatoma,
is the orientation of the ear canal in relation to the
attic. The image below shows a coronal computed tomographic
section through the temporal bone, which reveals that an
axis line drawn through the ear canal ends in the attic
rather than the mesotympanum. The only structure that is in
the way is the scutum, and its removal allows wide and open
access to the attic, which is the natural cul de sac of the
external auditory canal.
 The
use of the endoscope enables the surgeon to visualize past
the shaft of larger surgical instruments, such as drills and
curettes, and allows better visualization of structures that
are parallel to the axis of the microscope. It is usually
necessary to position structures such as the ear canal at a
right angle to the axis of the microscope for adequate
visualization. However, there are usually 2 issues of
feasibility that raise the most questions about the use of
the endoscope in ear surgery. The
use of the endoscope enables the surgeon to visualize past
the shaft of larger surgical instruments, such as drills and
curettes, and allows better visualization of structures that
are parallel to the axis of the microscope. It is usually
necessary to position structures such as the ear canal at a
right angle to the axis of the microscope for adequate
visualization. However, there are usually 2 issues of
feasibility that raise the most questions about the use of
the endoscope in ear surgery.
The first
consideration is the use of an endoscope of 4 mm, which is
large for the ear canal. During this author’s 10 years of
experience in performing endoscopic surgery on patients as
young as 3 years, that concern proved unfounded. In
addition, it is almost impossible to operate through a
smaller scope because the field of view that is essential
for orientation is lost. The second concern has arisen
because during microscopic transcanal surgery, many
otologists use one hand to hold the speculum and the other
hand to operate. This type of one-handed surgery, the lack
of suction, and the possibility of excessive bleeding can be
problematic. Also, prior experience in performing
postauricular procedures (in which many layers of tissue are
violated and a tremendous amount of healthy bone is removed
during cortical mastoidectomy) cannot be applied to the
transcanal endoscopic approach, in which surgically induced
trauma is quite limited, there is less bleeding, and the
dead-end structure of the canal and cavity allows for the
interim packing of certain areas to control bleeding. The
amount of bone removed is also limited to a relatively thin
scutum that is easily excised with a curette instead of a
drill.
 Some
experts in the otologic community have stated that the
transcanal approach to the removal of a cholesteatoma could
be performed with the aid of a microscope. The limited view
provided by the microscope is the main reason for which
those making such an argument cannot recall excising a
cholesteatoma via the transcanal approach over the last few
years. However, this author uses primarily the transcanal
approach for the removal of a cholesteatoma. Some
experts in the otologic community have stated that the
transcanal approach to the removal of a cholesteatoma could
be performed with the aid of a microscope. The limited view
provided by the microscope is the main reason for which
those making such an argument cannot recall excising a
cholesteatoma via the transcanal approach over the last few
years. However, this author uses primarily the transcanal
approach for the removal of a cholesteatoma.
Safety Concerns:
Two major safety concerns are
associated with endoscopic ear surgery: excessive heat
dissipation and secondary direct trauma from the tip of the
endoscope, which is caused by unintentional movement of the
patient. To avoid excessive heat dissipation that is
associated with the size of the cavity, adequate
illumination of the middle ear space can be accomplished
with the use of lower settings on a Xenon light source to
reduce heat. The tip of the endoscope also requires
continual cleaning with an antifog solution, which may cool
the endoscope. Although secondary direct trauma from the tip
of the endoscope remains a concern, the diameter (4 mm) of
the endoscope used by this author and the anatomy of the ear
canal and middle-ear space usually prevent the introduction
of the endoscope beyond the tympanic ring. Even during
endoscopic stapedectomy, there is less need for curettage of
the posterior and superior aspects of the canal to enable
exposure. This provides a protective rim that prevents the
advancement of the endoscope beyond the tympanic ring.
IWGEES
|